
Clavicle Non Union Case
A 64-year-old gentleman, was referred for assessment of a painful right clavicle nonunion.
His medical history was notable for previous complex clavicular pathology. He had undergone multiple surgical procedures beginning in 2011 for fixation of his right clavicle fracture using an intramedullary pin which became infected and went onto a nonunion where the clavicle does not heal. The pin in his clavicle was then removed and a second operation done with a plate to try to get his clavicle to heal. Despite these revision procedures, including the intramedullary fixation and plate stabilisation, he developed a persistent hypertrophic non-union and was left with a painful clavicle that never healed.
On examination he had a palable deformity in his collar bone that was painful and there was crunching and mobility over the site where the clavicle had not healed. He presented to see if there was anything that could be done for his nonunion that had occurred 14 years ago.
Subsequent imaging confirmed an established hypertrophic non-union of the right clavicle. CT scans and preoperative planning were arranged to assess the feasibility of surgical correction with bone grafting to restore clavicular length. A careful plan was put forward to possibly take down his nonunion, bone graft the defect and replate the clavicle.
This was all done with 3D CT imaging.
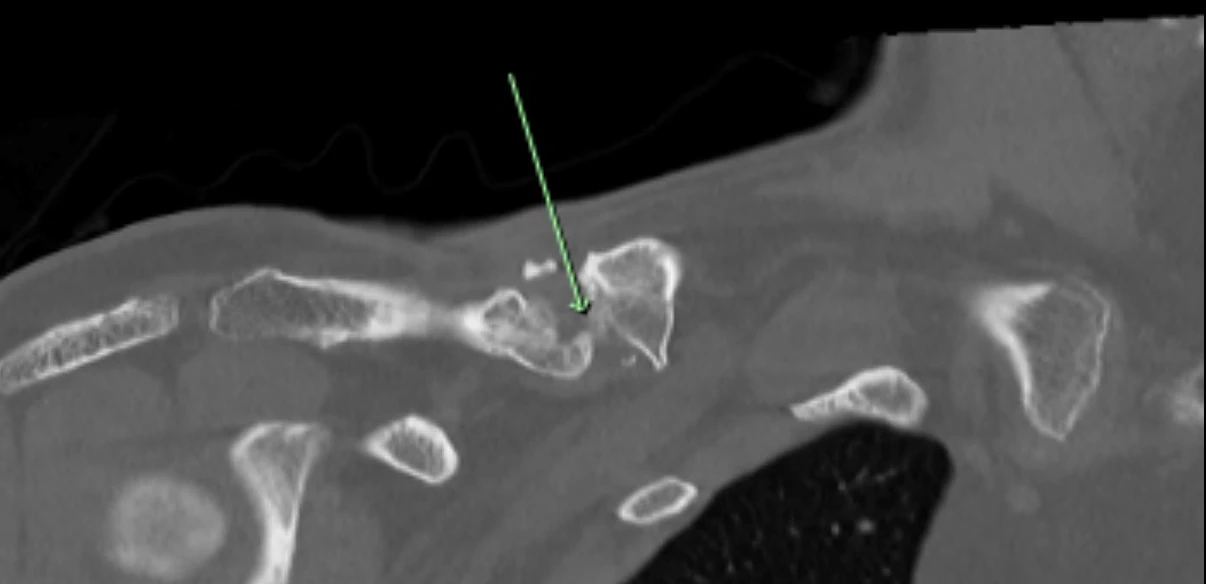
Pre op CT 1 showing site of non union
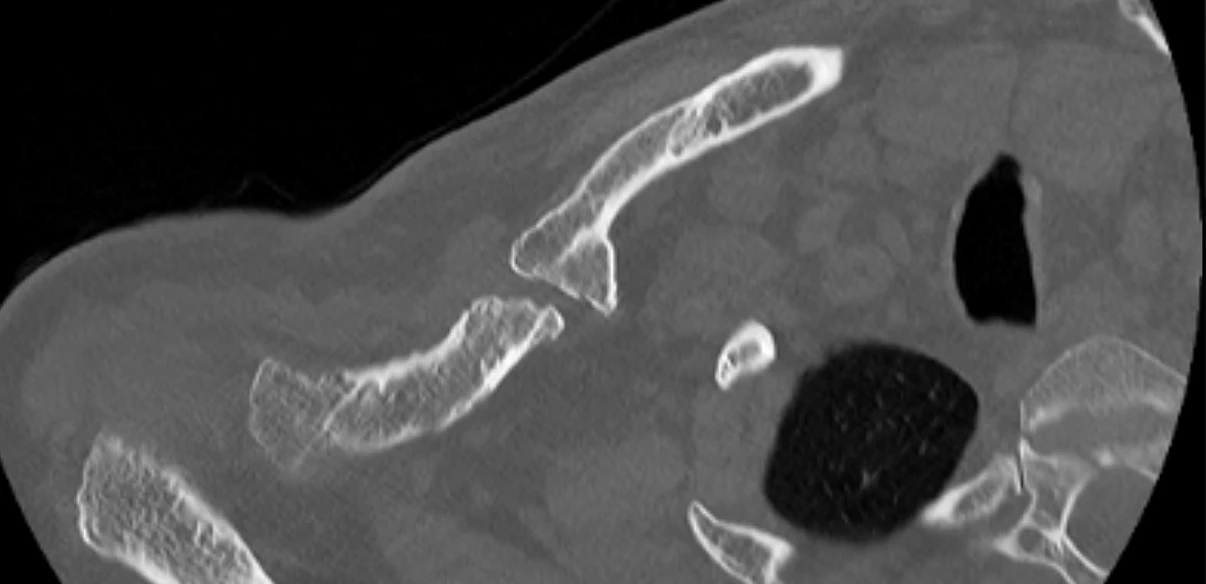
Pre op CT 2
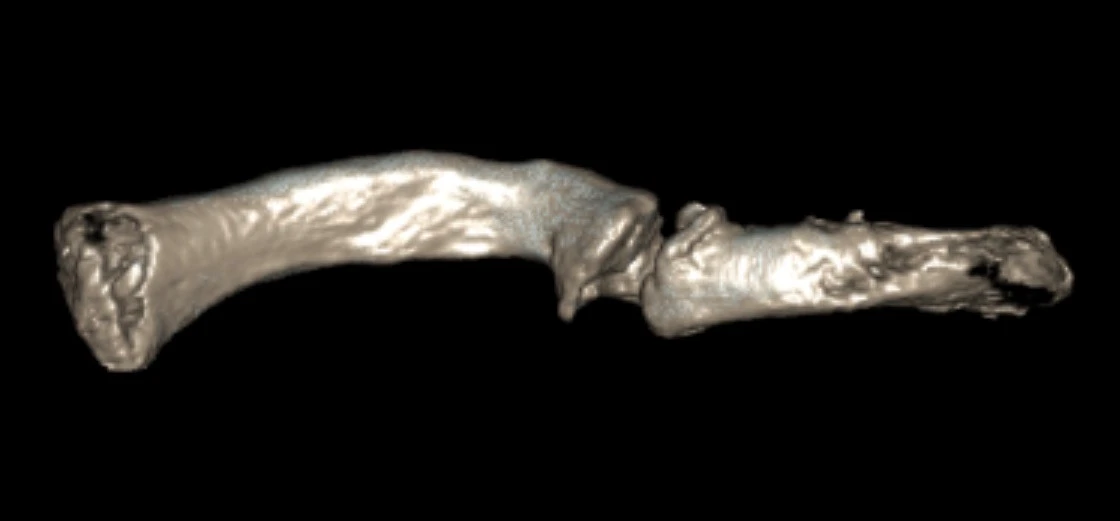
Pre op 3D model 1
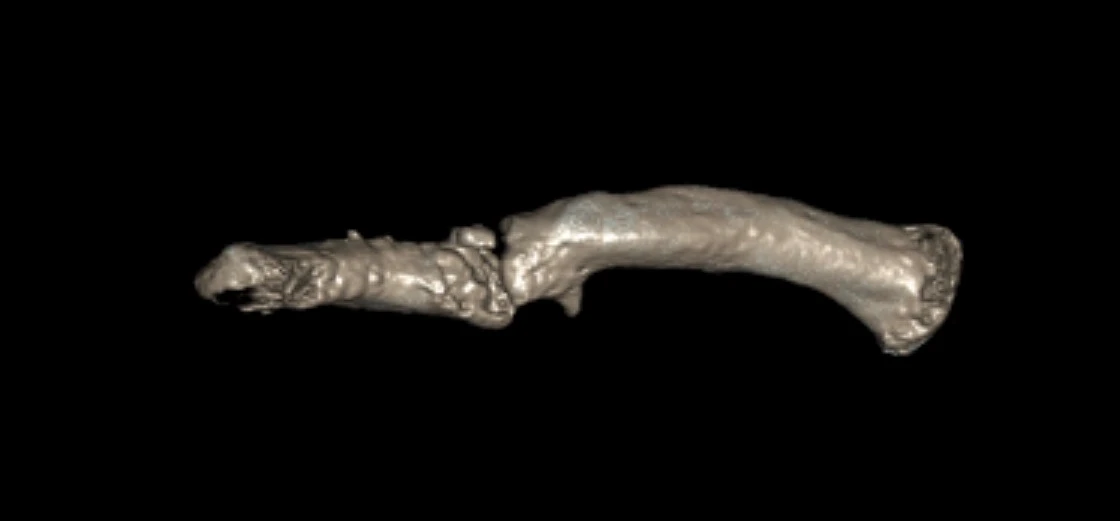
Pre op 3D model 2
On 28 August 2025, a revision open reduction and internal fixation of the right clavicle with iliac crest bone grafting was performed under general anesthesia.
The previous incision was reopened, and the non-union site was exposed. The bone ends were debrided to healthy bleeding bone. A structural iliac crest graft measuring approximately 1 x 1 cm was harvested from the right side and inserted between the clavicular fragments to restore length. A hybrid locking plate was applied, achieving excellent fixation and stability. Bone graft was packed around the non-union site. The wound was irrigated and closed in layers, and intraoperative swabs were taken to exclude infection.
Postoperatively, the patient received intravenous antibiotics for two days followed by oral antibiotics. Cultures were monitored for two weeks, and the arm was immobilised in a sling for one to two weeks. He then gradually started to move his arm.
The patient felt good at the initial postop visit and was feeling good at 6 weeks with minimal discomfort. He was told to use his arm as comfort allows but not to over do things.

Post op xray 1
At six-month review, radiographs demonstrated solid fracture union with restoration of clavicular alignment. Clinically, he had achieved full range of motion, complete resolution of deformity, and was entirely pain-free.

Post op xray 6 months
This case highlights the successful staged management of a chronic nonunion of the clavicle with iliac crest bone grafting. Through careful planning, meticulous surgical technique, restoration of clavicular length, rigid fixation, and autologous bone grafting, durable union and full functional recovery were achieved.
For specific advice regarding clavicle non-union surgery, please book an appointment with Dr David Duckworth on (02) 9806 3333