Clavicle Fractures in Adults
This article is based on the following published journal article:
Low AK, Duckworth DG, Bokor DJ. Operative outcome of displaced medial-end clavicle fractures in adults. J Shoulder Elbow Surg. 2008 Sep-Oct;17(5):751-4. doi: 10.1016/j.jse.2008.01.139. Epub 2008 May 21. PMID: 18499484.
Abstract
The results following nonoperative treatment of displaced, medial end clavicle fractures is often unsatisfactory; but no study has yet reported the outcome of operative fixation of these fractures. This study reports the results of open reduction and internal fixation on displaced, medial end clavicle fractures, in five adult patients (aged 25-52 years, mean 43) including 1 patient with a nonunion. The mean follow-up was 3.3 years (8 months-10.3 years). All fractures had united clinically and radiologically. No complications occurred, and no revision surgery was required. VAS pain scores averaged 0.75 (0-2) at rest, 0.75 (0-2) for normal activities, and 1.0 (0-2) for heavy activities. The mean DASH score was 9.0 (0-17), and all patients were very satisfied with the results of surgery (VAS 10). All patients had a full range of motion of their shoulder at final follow-up and were able to return to pre-injury occupational and activity levels.
Discussion
Five adult patients were identified who had operative treatment for a displaced medial end clavicle fracture. All were male with a mean age of 43 (25–52) years. Three were right-hand dominant, and in 4, the injury affected their dominant side. The cause was typically the result of a high energy injury (motorcycle 3, motor vehicle accident 1, rugby 1), and all were isolated injuries. Preoperative computed tomography (CT) scans were obtained in 2 patients to assess the amount of anterior displacement. The 3D reconstructions were able to define the deformity accurately in these patients.
In 4 cases, the fracture was acute and fixed within 2 weeks of the injury. One patient, however, presented with a painful, hypertrophic nonunion 9 months after the injury. This fracture was stabilized after taking down the hypertrophic nonunion and fixing the fracture with a plate, screws, and local bone graft.
The mean follow-up was 3.3 years (8 months-10.3 years). All fractures united clinically and radiographically. No complications occurred, and 1 patient had a second surgery for voluntary hardware removal 6 months after surgery, despite being asymptomatic. All patients had a full range of motion in the shoulder at last review. The mean VAS pain scores were 0.75 (0-2) at rest, 0.75 (0-2) with normal activities, and 1.0 (0-2) with heavy activities. The mean DASH score was 9.0 (0-17), and all patients were very satisfied with the results of surgery (mean VAS 10). All patients had managed to return to their previous occupation and activity levels.
Results
Indications for surgery on medial end clavicle fractures have traditionally only included open fractures, neurovascular involvement, or with a threat to the integrity of the overlying skin, even in the presence of significant displacement. Unsatisfactory results following nonoperative treatment of displaced, medial end fractures have influenced some surgeons to include these fractures as an indication for internal fixation. However, due to the rarity of this fracture, only 1 study to date has reported solely on medial end clavicle fractures, and none is available with results following operative fixation.
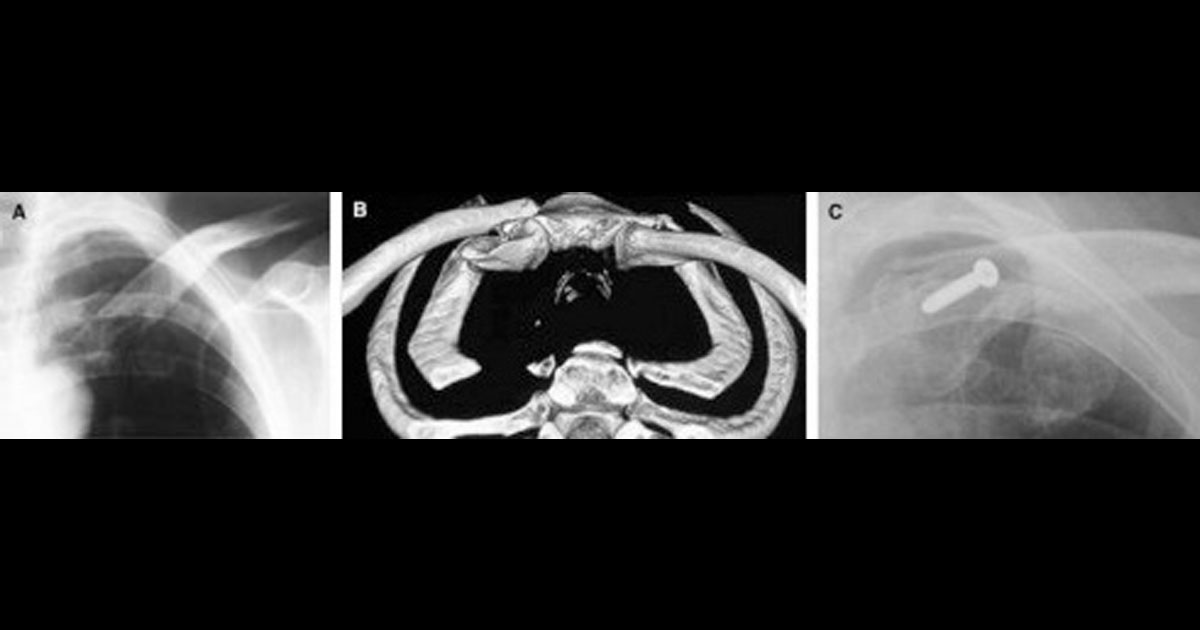
Recently, Throckmorton et al reviewed 57 medial end clavicle fractures retrospectively in 55 patients that presented to a level 1 trauma center. Treatment was nonoperative, except in 4 where an open fracture was present. The majority was the result of high energy trauma, such as motor vehicle accidents, and this finding was supported by our study and others. Ninety percent of their patients sustained multisystem injuries with an associated 20% mortality rate. Medial end fractures comprised 9.3% of all their clavicle fractures, a higher incidence than that reported previously. This was accounted for by the higher use of CT scans in the trauma setting, where 22% of fractures were seen only on CT scans, but not on radiographs. CT scans can also be useful for determining the amount of displacement, especially in the coronal plane, which may not be readily seen on chest x-rays alone (Figures 1 and 2). In their study, 44% of medial end fractures were minimally displaced (<2mm), 23% had 2-10 mm, and 33% had >10 mm of displacement. Disappointingly, after a mean of 15.5 months, the majority of patients still reported mild (25%), moderate (22%), or severe (6%) pain.
The nonunion rate following nonoperative treatment of medial end fractures is difficult to determine, as studies have been limited by the small number of patients in reported series. However, most studies have suggested a poorer outcome when displaced medial end fractures are treated nonoperatively. In a prospective series of 222 consecutive clavicle fractures, fracture displacement was found to be the strongest radiographic risk factor for sequelae. The authors identified 4 (2%) medial end fractures, and after 6 months, half of these (2 patients) still complained of weakness and pain at rest and with activity. One patient had a nonunion. In a prospective study of 868 consecutive clavicle fractures treated nonoperatively, only 24 (2.76%) involved the medial end with the rate of nonunion higher for displaced (14.3%) than for nondisplaced fractures (6.7%). In contrast, one study reported good results with nonoperative treatment. In 1000 consecutive clavicle fractures, all medial end fractures (n ¼ 28, 2.8%) united with only one requiring later surgery for a bony prominence. However, only 5 fractures had been considered displaced. In both of these studies, the authors concluded that fracture displacement significantly increases the risk of delayed and nonunion for diaphyseal and lateral end clavicle fractures, but the numbers were too small to make conclusions on medial end fractures.
The treatment of clavicle nonunions can be challenging, and the literature is sparse in this area. In a series of 20 clavicle nonunions,1 the only medial end nonunion healed after internal fixation with a lag screw and bone graft. However, the patient still complained of severe pain after 32 months. In our study, the patient who had fixation of a nonunion did very well after 8 months of follow-up. He complained of no pain other than with heavy lifting, had a full range of shoulder movement, and had returned to full-time work. In conclusion, although limited by the small number of cases, our study has shown that early fixation of displaced medial end clavicle fractures can result in anatomic reconstruction of the clavicle and a favorable outcome with minimal complications as measured using VAS and DASH scores.
References
For specific advice regarding clavicle fractures, please book an appointment with Dr David Duckworth on (02) 9806 3333